

Background
Thalassemia Syndromes (TS) are commonly classified as transfusion-dependent-thalassemia (TDT) or non-transfusion-dependent thalassemia (NTDT) at diagnosis on the basis of requirement for lifelong regular transfusion therapy for survival. However, data from observational studies and expert opinion suggest that these categories may reflect a wide spectrum rather than a dichotomy, and may actually be interchangeable at many parts of the disease journey. Thus, an evaluation of alternate clusters to classify TS patients remains of merit.
Aims
The aim of this study was to cluster TS patients on the basis of possible clinical indicators of phenotype severity (IPhS) using suitable algorithms and to determine whether these are able to detect cohorts with different clinical phenotypes.
Methods
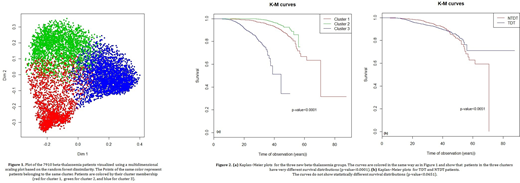
Representatives from thirteen international centers from seven countries agreed on 19 IPhS to be collected for a retrospective study. Data from 7910 TS patients were collected. NbClust R Packagewas performed for exploring the existence of a substructure inside the studied TS population, determining the best number of clusters. Unsupervised Random Forest (RF)clustering and the Partitioning Around Medoids (PAM)algorithms were performed to define the clusters. The most important IPhS in defining clusters were selected according to the Gini index. Kaplan-Meier (K-M) survival curves of the identified clusters, defined by the selected IPhS, were used to represent the risk of death for these clusters.
Results
NbClust method showed the existence of three possible clusters. The RF-PAM procedure defined three distinct clusters with a classification error rate of 4.3% (Fig 1). Moreover, the most important IPhS were patient age, mean serum ferritin level, age at diagnosis, age at first transfusion, age at first iron chelation, and number of complications. K-M curves showed statistically significant differences in survival among the three clusters (p<0.0001,Fig 2a) but not between the original classification of NTDT and TDT (p=0.0651, Fig 2b).
Conclusions
The observation of statistically significant differences in survival between the three newly identified clusters but not the original TDT-NTDT classification confirms that the latter classification is interchangeable, and a new triad classification system is required. These findings warrant further evaluation in prospective studies to determine specific thresholds for IPhs indicators that can aid physicians in assigning classes and tailoring care, in order to improve survival in TS patients.
Meloni:Chiesi Farmaceutici S.p.A.: Other: speakers' honoraria. Pistoia:Chiesi Farmaceutici S.p.A.: Other: speakers' honoraria. Vichinsky:Novartis: Consultancy, Research Funding; Bluebird Bio: Consultancy, Research Funding; Agios Pharmaceuticals: Consultancy, Research Funding; Pfizer: Consultancy, Research Funding; GBT: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal